- Pediatric Dentistry Guide · For Parents · Williamsburg
Your dentist said “baby root canal” and your stomach dropped. Here’s what a pulpotomy actually is, why it’s far less dramatic than it sounds, and what to expect step by step.
Does My Child Really Need a Pediatric Root Canal? A Parent's Guide
Your child has been up through the night with tooth pain. Or your pediatric dentist just mentioned the words “baby root canal” at a routine checkup — and your stomach dropped a little. Both reactions are completely understandable. But a pediatric root canal sounds more alarming than it usually is.
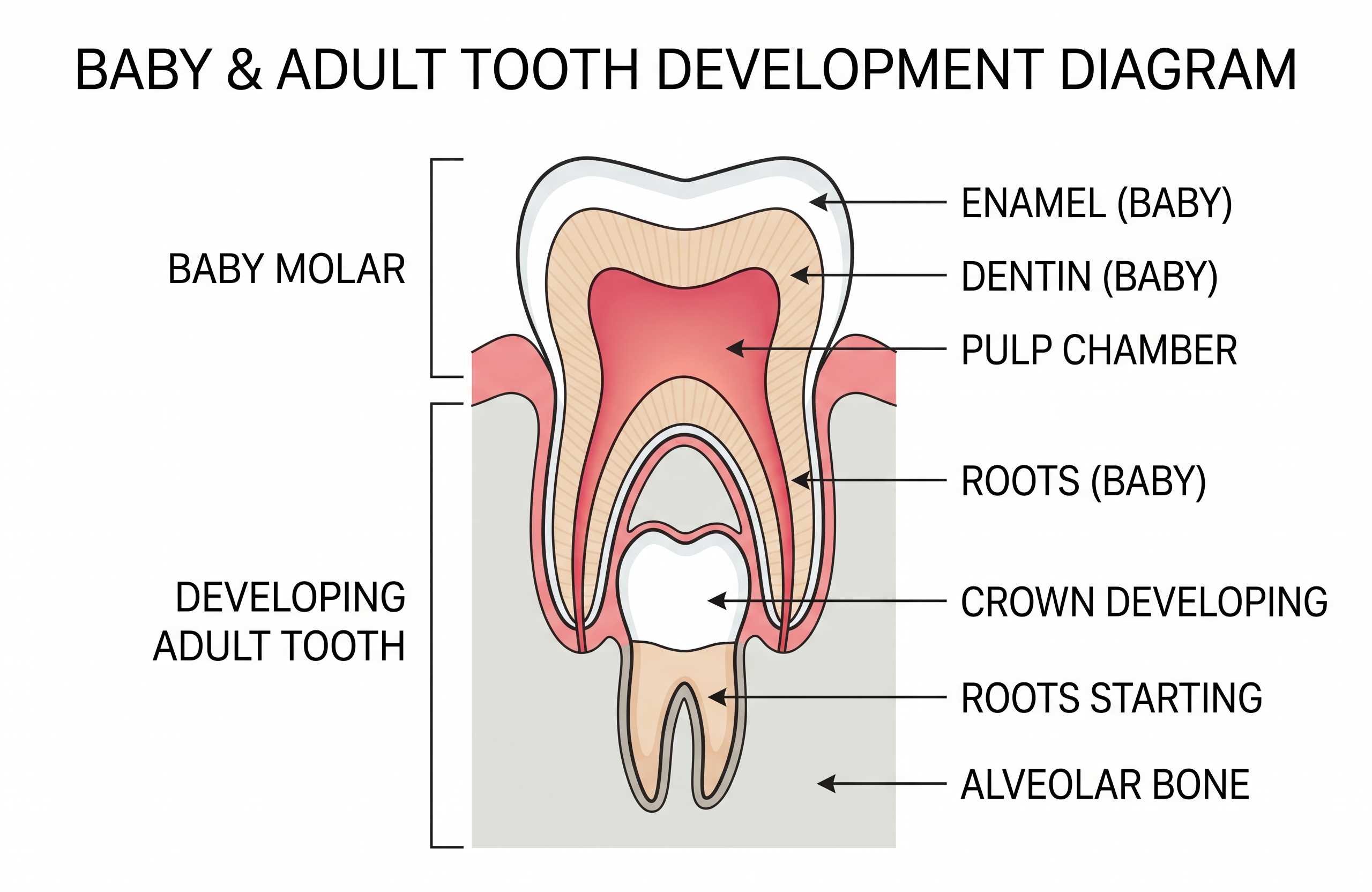
The procedure most commonly recommended for young children is actually a pulpotomy — a gentler, more limited treatment than the adult version most parents picture. When a primary tooth has decay that has reached the pulp (the soft tissue inside the tooth containing nerves and blood vessels), a pulpotomy removes the infected portion of that tissue rather than the entire pulp structure. The goal is to save the tooth, relieve the pain, and protect the underlying permanent tooth that is still developing beneath it.
WHAT IS A PULPOTOMY?
A pulpotomy removes only the infected pulp in the crown (top portion) of the baby tooth — not the roots. This is why it’s usually quicker and less involved than the adult root canal most parents are imagining. It’s one of the most common pediatric dental procedures.
Why We Must Save a Baby Tooth with a Pulpotomy
It’s a common question from parents: if the tooth will fall out anyway, why not just pull it? The short answer is that back baby teeth do important work for years — often until ages 10–12 for back molars. Pulling them early creates real problems.
- Chewing & Nutrition
Primary molars handle most chewing in childhood. Losing them early can make eating harder and significantly limit food choices during key developmental years.
- Speech Development
Teeth help children form certain sounds. Early tooth loss can affect speech clarity while speech patterns are still developing and forming.
- Space for Adult Teeth
Primary molars hold the space for the adult tooth underneath. If removed too early, nearby teeth drift — often leading to crowding and orthodontic treatment later.
- Bone & Tissue Preservation
Keeping the tooth helps maintain the bone and gum support in that area until the permanent tooth is ready to erupt naturally.
Pulpotomy vs. Extraction vs. Adult Root Canal
| Option | What Happens | Goal & Typical Follow-Up |
|---|---|---|
|
Pulpotomy
Baby root canal
|
Infected pulp in the crown of the tooth is removed; a medicated mineral-based filling is placed to protect the remaining healthy tissue | Save the baby tooth and restore function; crown typically placed the same appointment or soon after; tooth held in place until it falls out naturally |
|
Extraction
Tooth removal
|
The primary tooth is removed under local anaesthetic; straightforward when the tooth cannot be restored or infection is too advanced | Eliminate infection quickly; a space maintainer is often needed to hold the gap until the permanent tooth erupts — without one, nearby teeth can drift and cause crowding |
|
Adult Root Canal
For permanent teeth
|
Full pulp removed — including the root canals; canals are shaped, cleaned, and sealed; a different and more involved process than a pulpotomy | Save a permanent tooth for life; typically followed by a crown; not the same procedure as a pulpotomy — and generally longer and more complex |
WHEN EXTRACTION MAY BE RECOMMENDED INSTEAD
A pulpotomy isn’t always the best option. If the tooth can’t be restored — because decay is too extensive, infection has affected surrounding bone, or there isn’t enough healthy tooth left to rebuild — extraction may be recommended. Your dentist should explain why they’re recommending extraction vs. saving the tooth. It’s reasonable to seek a second opinion for major decisions.
Tooth decay that is still in the outer layers of a tooth rarely causes significant pain. When decay reaches the pulp, the symptoms change — and they tend to be hard to miss.
Toothache that wakes your child at night or is persistent rather than occasional
Sharp or lingering sensitivity to hot, cold, or sweet foods and drinks
Spontaneous pain — throbbing or sharp pain without any food or drink trigger
A small pimple or bump on the gum near a tooth — this may be a dental abscess draining
Swelling of the gum or face near the affected tooth
A persistent bad taste in the mouth that your child mentions
Refusal to chew on one side of the mouth
Visible darkening of a tooth that was previously a normal colour
Fever accompanying dental symptoms
What Is a Dental Abscess and Why Does It Matter?
A dental abscess is a pocket of infection that forms when decay reaches the tooth’s nerve and spreads into nearby tissue or bone. In children, it may show up as a small pimple-like bump on the gum (a draining fistula). Even if that bump seems to reduce pain — it doesn’t mean the infection is gone. It means it’s still active and draining.
Dental infections don’t resolve on their own. Without treatment, they can spread to nearby teeth and bone and may affect the developing adult tooth underneath.
When to Call 911 or Go to the ER Instead
Facial or neck swelling that is spreading , especially toward the jaw, eye, or throat
Difficulty breathing or swallowing — this is a medical emergency, not a dental emergency
High fever alongside significant facial swelling
Swelling that changes rapidly over hours rather than days
Many parents worry about how their child will handle a pulpotomy — especially if they’re anxious or had a tough dental experience before. Here’s what typically happens during the appointment, and how the visit is kept as calm and comfortable as possible.

EXAM & X-RAYS
The dentist examines the tooth and uses X-rays to confirm how deep the decay is and whether the tooth is a good candidate for a pulpotomy rather than extraction.
NUMBING THE AREA
Local anaesthesia numbs the tooth and gums. Your child may feel pressure, but shouldn't feel pain. A topical numbing gel is often applied first to make the injection more comfortable.
NITROUS OXIDE (IF APPROPRIATE)
For anxious or very young children, nitrous oxide ("laughing gas") may be offered if clinically appropriate. It's gentle, wears off quickly, and most kids return to normal activities the same day. Availability depends on your child's age, health, and the practice.
ISOLATION & DECAY REMOVAL
A rubber dam or similar isolation keeps the area dry and prevents swallowing materials. The dentist removes decay and accesses the pulp chamber.
REMOVING THE INFECTED TISSUE
Only the infected pulp in the crown of the tooth is removed — not the full root canals like an adult root canal. This is why pulpotomies are usually quicker than parents expect.
MEDICATED FILLING
A medicated, mineral-based material is placed to protect the remaining healthy tissue and seal the tooth against bacteria re-entering the space.
CROWN PLACEMENT
In many cases, a crown is placed the same day — or soon after — to protect the treated tooth from fracture and seal it fully until it falls out naturally.
Parent Preparation Checklist
Light meal beforehand:
Comfort item:
Medical history & allergies:
Arrive early:
Use calm, neutral language:
Aftercare: What to Expect in the First 24–48 Hours
PAIN MANAGEMENT
Mild soreness after the anaesthesia wears off is normal. Use children’s OTC pain relief only as directed on the label or by your pediatrician/dentist. Do not place aspirin directly on the gums.
SOFT FOODS (1–2 DAYS)
Avoid hard, crunchy, or very chewy foods while the area is tender. Yogurt, scrambled eggs, soft pasta, and similar foods are ideal for the first day or two.
GENTLE BRUSHING
Continue gentle brushing that evening, being careful around the treated tooth. Stopping brushing is not necessary and not recommended.
WHEN TO CALL THE OFFICE
Call if pain worsens after the first 24 hours — rather than improving — or if you notice new swelling, fever, or a visible change in the gum near the treated tooth.
Pediatric Crowns: Protecting the Restored Baby Tooth

After a pulpotomy, a dental crown is typically placed over the treated tooth. For many parents, this is an unexpected part of the treatment plan — especially if a crown was not initially mentioned. After the infected pulp tissue is removed and a medicated filling placed, the tooth structure that remains is significantly more fragile and needs protection.
Protects from Fracture
The treated tooth is more fragile under chewing pressure. A crown prevents fracture that could lead to early, unplanned extraction.
Seals Against Bacteria
The crown creates a tight seal that prevents bacteria from re-entering the pulp space and causing a new infection.
Extends the Tooth's Life
Keeps the tooth functional and space-holding until the permanent tooth naturally replaces it — often ages 10–12 for back molars.
Reduces Re-Treatment Risk
Properly crowned teeth require less follow-up emergency treatment than uncrowned pulpotomies, saving stress and appointments.
WHAT TYPE OF CROWN?
The most common option for treated baby molars is a stainless-steel crown — a durable metal cap that covers the whole tooth and is often placed in one visit. It sits on back teeth where it’s rarely visible. Some offices also offer tooth-coloured crowns for certain cases. A stainless-steel crown is designed to last until the baby tooth falls out naturally — care is simple: brush normally, floss when possible, and keep up with routine cleanings.
Prevention: Protecting All the Other Teeth
A pulpotomy treats one tooth — but the goal for the rest is prevention. These habits make the biggest difference between routine checkups and repeated dental emergencies.
Brush twice daily with fluoride toothpaste
Adult-assisted brushing until around age 7–8
Reduce sugar frequency, not just amount
Routine dental checkups every 6 months
Frequently Asked Questions
Why do kids need a root canal on a tooth that will fall out anyway?
What is the difference between a baby pulpotomy and an adult root canal?
Is a pediatric root canal safe for a toddler?
Will my child be put to sleep for a pulpotomy?
How much does a child's root canal and crown cost in NYC?
Can a baby tooth infection damage the permanent tooth underneath?
How can I manage my child's severe tooth pain at home safely?
What happens if a parent refuses a baby root canal treatment?
Early Treatment Is Almost Always the Simpler Path
A “pediatric root canal” — usually a pulpotomy — is often less involved than it sounds. In a calm, child-friendly setting, most kids do well, recover quickly, and keep the tooth working for years. What matters most is timing. Treating decay early is almost always simpler than treating an abscess that’s had time to spread. If your child has nighttime tooth pain, sensitivity, or swelling — don’t wait.
IS YOUR CHILD IN TOOTH PAIN?
Don’t wait for the pain to get worse. Book a kids’ dental exam at Toothology in Williamsburg — we’ll assess the tooth, take X-rays, and explain your options clearly.
DIRECT LINE
IN THIS GUIDE
QUICK DECISION GUIDE
Facial or neck swelling spreading toward the jaw, eye, or throat → Go to the ER.
TOOTHOLOGY DENTAL
Williamsburg, Brooklyn, NY
Serving Greenpoint, Bushwick, Bed-Stuy & Downtown Brooklyn
718-678-3800
Emergency line available
Open Hours
Mon – Thu: 10:00 AM – 6:00 PM Friday: 10:00 AM – 2:00 PM Sunday: 10:00 AM – 2:00 PM Saturday: Closed
OUR COMMITMENT
- Board-Certified Pediatric Dentists
- Child-Friendly, Anxiety-Reducing Care
- Same-Day Emergency Slots
- Low-Radiation Digital X-Rays
- Most Major Insurance Accepted