- Wisdom Teeth Removal Guide · Williamsburg · 3D Imaging
CBCT 3D imaging shows the exact path of the nerve, root shape, and jaw anatomy that a flat 2D X-ray can’t. Here’s why it changes the surgical plan — and what recovery actually looks like.
Wisdom Teeth Removal in Williamsburg: How 3D Imaging Makes Surgery Safer
For most people, wisdom teeth removal is something they know is coming long before it becomes urgent. A dentist mentions it at a routine checkup. An X-ray shows third molars heading in the wrong direction. Or the jaw starts aching in a way that feels different from anything before. Then comes the question most people delay longer than they should: when is the right time, and how do I make sure this goes as smoothly as possible?
Wisdom teeth removal is one of the most commonly performed dental procedures, and for the vast majority of patients it goes without significant complication. But the cases that generate the most anxiety, and the most serious post-operative concerns, often involve anatomy that isn’t fully characterised on initial 2D imaging — especially when roots appear close to important nerves. Modern CBCT 3D imaging has changed that picture significantly.
Why 3D Nerve Mapping Is Essential for Safe Third Molar Extraction
The inferior alveolar nerve — which supplies sensation to the lower lip, chin, and lower teeth — runs in a canal in the lower jaw near the roots of lower wisdom teeth. In simple, fully erupted cases, a panoramic X-ray may be enough. But with deep impactions or roots that appear close to the nerve on a 2D image, there can be real uncertainty.
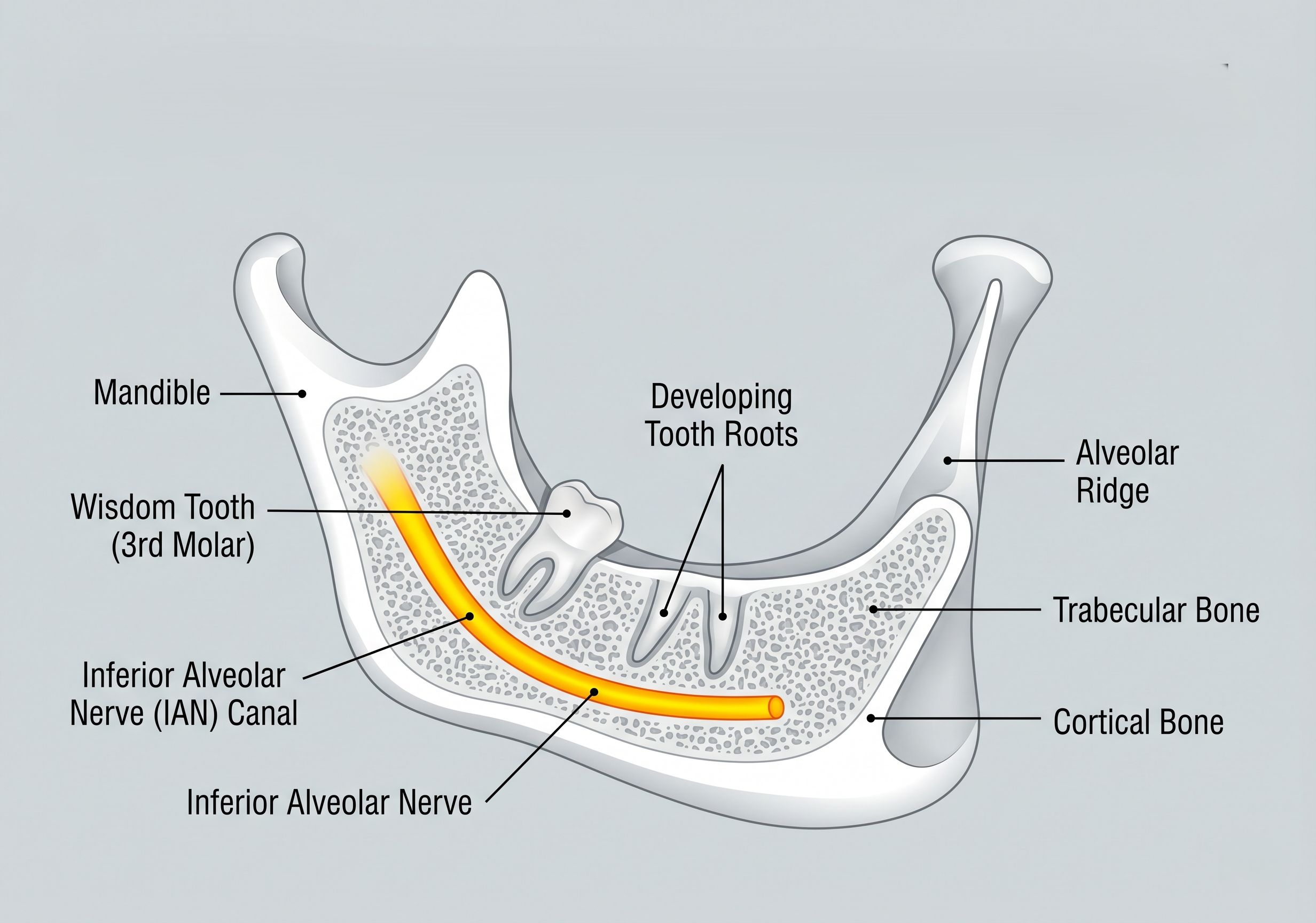
A CBCT (cone beam CT) 3D scan gives a full three-dimensional view of the jaw so the surgeon can see the exact relationship between the roots and the nerve canal — information that can directly affect the surgical plan.
Whether to Section the Tooth
Removing the tooth in smaller pieces can reduce force near nerve-adjacent roots. CBCT helps guide that decision more precisely than a flat image can.
Which Approach to Use
3D mapping can influence the entry angle, how much bone needs to be removed, and the safest direction of controlled pressure during extraction.
Whether to Refer
CBCT may reveal complexity that is better handled by a specialist — far better to know before surgery than to discover it mid-procedure.
Sinus Proximity (Upper Teeth)
For upper wisdom teeth, 3D imaging maps the floor of the maxillary sinus precisely — helping avoid sinus communication during extraction.
IMPORTANT CLARIFICATION: IMAGING REDUCES RISK — IT DOES NOT ELIMINATE IT
A CBCT scan is a planning tool, not a guarantee. If a wisdom tooth sits close to the inferior alveolar nerve, there is still some risk of temporary tingling or numbness in the lower lip or chin. In most cases, these sensory changes improve as the nerve heals, and permanent injury is rare. What CBCT does is give the clearest possible view of your anatomy so the surgeon can plan the most precise, nerve-aware approach.
What CBCT Shows That a Panoramic X-Ray May Not
| Imaging Capability | Panoramic X-Ray | CBCT 3D Scan |
|---|---|---|
| View Dimension | 2D flat image — one perspective only | Full 3D volumetric view from any angle |
| Nerve Path Visualisation | General proximity only — nerve appears as a line on the image | Precise 3D path of the inferior alveolar nerve relative to each root tip |
| Root Shape & Anatomy | Overlapping roots can be ambiguous or misleading on a flat image | Each root tip and its exact position shown clearly in three dimensions |
| Depth & Angulation | Limited — bucco-lingual (front-to-back) depth cannot be assessed | Full depth and exact angulation of each root visible in all planes |
| Adjacent Structure Mapping | Maxillary sinus proximity is only approximate | Sinus floor, adjacent teeth, and bone density all visible and measurable |
| Surgical Planning Impact | Sufficient for straightforward, fully erupted teeth | Enables modified surgical approaches for high-risk nerve proximity cases |
| Radiation Level | Lower dose; commonly used as the initial screening image | Higher than panoramic but typically lower than medical CT; used when 3D detail is clinically warranted |
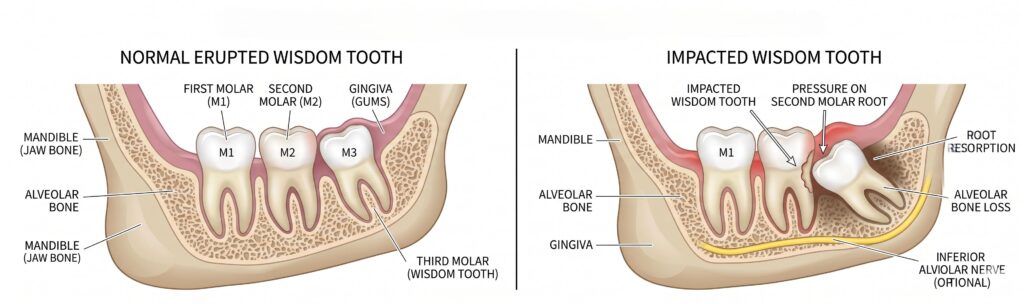
Wisdom teeth don’t have to be fully impacted to cause problems. Even partially erupted or misaligned third molars can generate a constellation of symptoms that, if left unaddressed, lead to damage extending well beyond the wisdom tooth itself.
Jaw pain or persistent deep aching — often worse at night or when chewing
Swelling or tenderness in the back gum — pericoronitis that keeps coming back
Bad taste or bad breath in one spot — food and bacteria trapped behind a partially erupted tooth
Headaches or jaw tension — impaction pressure can contribute to jaw and temple headaches
Repeated gum infections — antibiotics may calm a flare-up, but recurrence usually means extraction
Damage to the second molar — impacted wisdom teeth can cause decay or root resorption on the adjacent molar
Bone loss near the second molar — X-rays may show bone breakdown or deep pocketing between the two teeth
Difficulty or discomfort opening the mouth — especially with swelling or infection present
WHEN THE DECISION CANNOT WAIT
Watching an impacted wisdom tooth can be reasonable when it is truly symptom-free — but that window often closes once the second molar starts showing bone loss or root resorption. That can become a bigger problem than the extraction itself.
Go to the ER or Urgent Care Immediately If You Have:
Swelling spreading to the throat, neck, or floor of the mouth
Difficulty breathing or swallowing
High fever with significant facial swelling
Inability to open the mouth (severe trismus), especially with systemic symptoms
Dental anxiety around wisdom tooth surgery is extremely common — especially when the tooth is impacted, may need sectioning, or sits near a nerve. Comfort options such as nitrous oxide and IV sedation are typically discussed before surgery. The best choice depends on the procedure, your anxiety level and medical history, what the office offers, and day-of logistics.
| Option | Advantages | Considerations | Best Suited For |
|---|---|---|---|
|
LOCAL ONLY LOCAL ANAESTHESIA ONLY |
No systemic effects; fastest recovery; can drive yourself home; full control | You are fully awake and aware during the procedure; not ideal for high anxiety | Simple extractions; low-anxiety patients; strong pain tolerance |
|
NITROUS NITROUS OXIDE (LAUGHING GAS) |
Mild relaxation; wears off within minutes; patients can typically drive; clinician adjusts level continuously | Still partially aware; not deep sedation; not appropriate for all patients or all procedures | Mild anxiety; straightforward procedures; patients who want to remain conscious but calmer |
|
IV SEDATION IV SEDATION (WHERE AVAILABLE) |
Deep relaxation or sleep-like state; little to no procedure memory; strong anxiety control | Requires a driver home; fasting beforehand required; longer post-procedure monitoring; full medical screening | High dental anxiety; complex or multiple extractions; strong gag reflex; patients who want to remember nothing |
WHAT SEDATION DOES NOT DO
Nitrous oxide reduces anxiety and makes treatment feel easier, but you’re still generally aware. IV sedation creates deeper, sleep-like relaxation and many patients remember little — but it’s not the same as hospital general anaesthesia. In all cases, sedation is paired with local anaesthesia so the area being treated stays numb. A medical history review is always part of sedation planning — heart or lung conditions, certain medications, and overall health can affect which options are safest.
Reducing Post-Op Swelling: The First 48 Hours After Surgery
The first 48 hours after wisdom teeth removal are when most of the acute swelling and discomfort occur — and also when the choices you make have the greatest impact on whether recovery is smooth or complicated.

- Do These Things
- Apply ice to the outside of the cheek — 20 minutes on, 20 minutes off for the first 24 hours
- Keep your head elevated, especially when resting — this reduces blood pooling and swelling
- Take any prescribed medications or OTC pain relief as directed by your dentist
- Eat soft foods: yogurt, mashed foods, smoothies without a straw, cooled soup
- Stay hydrated with water; sip gently rather than gulping
- Gently rinse with warm salt water after 24 hours, as directed by your dentist
- Avoid These Things
- Straws — the suction can dislodge the blood clot and cause dry socket
- Smoking or tobacco — significantly increases dry socket and infection risk
- Spitting or forceful rinsing in the first 24 hours
- Hard, crunchy, or chewy foods that require significant biting force
- Vigorous physical activity or exercise for at least 48 hours
- Probing the extraction site with your tongue or fingers
Dry Socket and the Swelling Timeline
Understanding Dry Socket (Alveolar Osteitis)
Dry socket happens when the blood clot in the extraction site comes out or breaks down too early, leaving bone exposed. It causes strong, throbbing pain — often radiating toward the ear — usually starting around day 3, after the initial soreness should be improving.
It’s the most common complication after wisdom tooth removal, but good aftercare lowers the risk significantly. The biggest triggers are smoking or tobacco use, using straws, vigorous rinsing or spitting, and poor cleaning around the area. Following your recovery “do-not” list prevents most cases.
If pain is getting worse rather than better around day 3, call the office. Dry socket is treatable — early attention makes it much easier to manage.
Swelling & Bruising: What to Expect
Hours 0–24
Ice phase · Begin swelling
48–72 Hrs
Swelling peaks here
Day 3–5
Bruising appears
~Day 7
Most swelling improved
1–2 Weeks
Bruising fades
SWITCH FROM ICE TO HEAT AFTER 24 HOURS
Ice in the first 24 hours can reduce initial swelling — apply 20 minutes on, 20 minutes off. After the first day, moist heat (a warm, damp cloth) can help swelling resolve more quickly. Contact your dental team if bruising spreads rapidly or comes with worsening swelling after day 3.
Frequently Asked Questions
How does a 3D CBCT scan reduce the risk of nerve injury during extraction?
What is the average price of removing four impacted wisdom teeth in NYC?
At what age should you get your wisdom teeth extracted?
What are the chances of getting dry socket after wisdom tooth surgery?
Can wisdom teeth push your other teeth out of alignment?
How long does the swelling last after an impacted tooth removal?
Does a basic PPO dental insurance cover wisdom teeth surgery?
What soft foods can I eat safely during wisdom teeth recovery?
Better Imaging, Better Planning, Better Recovery
Wisdom teeth removal is usually simplest before infection or second-molar damage has started. With CBCT imaging when needed and comfort options like nitrous or IV sedation, your plan can be precise and predictable. If you’ve had pain, swelling, or repeat flare-ups — don’t wait.
WISDOM TOOTH PAIN OR SWELLING?
Book a consultation at Toothology in Williamsburg — we’ll assess your anatomy with imaging and give you a clear, honest plan before any commitment.
DIRECT LINE
IN THIS GUIDE
QUICK DECISION GUIDE
Swelling spreading to throat or neck, difficulty breathing → ER immediately.
TOOTHOLOGY DENTAL
Williamsburg, Brooklyn, NY
Serving Greenpoint, Bushwick, Bed-Stuy & Downtown Brooklyn
718-678-3800
Emergency line available
Open Hours
Mon – Thu: 10:00 AM – 6:00 PM Friday: 10:00 AM – 2:00 PM Sunday: 10:00 AM – 2:00 PM Saturday: Closed
OUR COMMITMENT
- Board-Certified Pediatric Dentists
- Child-Friendly, Anxiety-Reducing Care
- Same-Day Emergency Slots
- Low-Radiation Digital X-Rays
- Most Major Insurance Accepted